
Oct 22, 2014
In the first part of this series, we took a look at the disease of Ebola itself. In the second installment we looked at the disease’s signs and symptoms, and took at look at how we as prehospital providers could be put at risk. In this final part we take a look at the role EMS will be paying in the battle against Ebola.
The EMS Response to Ebola

Spanish paramedics doing it the right way.
In a recent EMS1 article, Dr. Alex Garza took a look at Ebola and how it will affect EMS responders. One of the first things that he pointed out was the need for specialized air ambulances to transport these patients. Personally, I feel that we need specialized responders as well. Dealing with highly infectious diseases such as Ebola requires specialized training and treatment for the patients. The infection control training that EMTs and paramedics receive is usually focused on “universal precautions and Body Substance Isolation” heck, if you don’t say that at the start of every National Registry station, you’re most likely going to have to retest, but I digress. . . Much like we have specialized HazMat technicians in many systems, and SWAT medics maybe we need specially trained medics and EMTs to handle specifically the interfacility transport of potentially contagious patients.
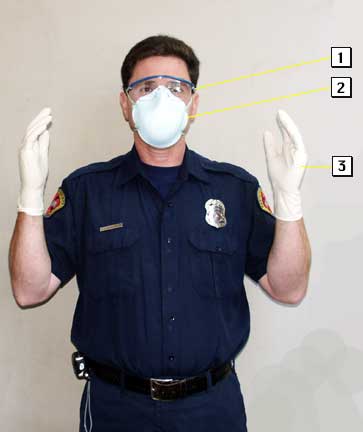
Typical personal protective equipment for EMS. Credit: Santa Clara County FD.
I also spend a lot of time reading the National EMS Management Association (NEMSMA) ListServ on Google. There has been a lot of talk over the past couple of weeks about different services developing policies and procedures for dealing with patients who possibly have contracted Ebola. If your department releases anything, read it. Memorize it. Make sure you know what your point of entry plan is. Is one hospital being designated as an Ebola receiving facility? Who do you have to notify if you have a possibly infected patient? Are there any radio codes that you need to be aware of? Also do not be afraid to ask your leadership for answers to any of these questions. If they don’t have them, suggest that they might be important. If they’re resistant go higher up the chain if you have to, or at least as high as you are comfortable going.
The Center for Disease Control and Prevention (CDC) has also given us some good guidance about how to deal with Ebola patients. Their system starts with classification. For example: a person is considered “under investigation” (PUI) when they have “both consistent symptoms and risk factors as follows”
- Clinical criteria, which includes fever of greater than 38.6 degrees Celsius or 101.5 degrees Fahrenheit, and additional symptoms such as severe headache, muscle pain, vomiting, diarrhea, abdominal pain, unexplained hemorrhage; AND
- Epidemiologic risk factors within the past 21 days before the onset of symptoms, such as contact with blood or other body fluids or human remains of a patient known to have or suspected to have (Ebola); residence in – or travel to – an area where (Ebola) transmission is active; or direct handling of bats or non-human primates from disease-endemic areas.
So a patient who fits the first criteria might be at risk, but they might also have the flu, or something else not at all related to Ebola. Remember: you need BOTH met for a person to meet the CDC’s criteria for a person under investigation.
Cleaning Up

Germicidal wipes. Your second best weapon in the battle against Ebola. The best one is common sense.
Another discussion that arose over the last week or two on the NEMSMA ListServ revolved around proper decontamination of an ambulance after contact with an Ebola patient. According to the CDC, you can use a virocide that is effective against Norovirus, Poliovirus, and Rotavirus. Many cleaning agents commonly found in ambulances cover at least two of these three. One poster, however, was quick to point out that the list the CDC refers people to via the Environmental Protection Agency (EPA) is close to 6 years old.
It seems though that the general consensus of most departments is they thoroughly wipe down and spray down all patient care surfaces, something that many of us could pay a lot more attention to. Also, it might be wise to leave your food outside the truck if at all possible, and avoid eating anywhere in the ambulance. I know that many live by this rule, but now is a great time to reinforce it.
Are we Being Over-Protective?
While some will say that there are many things out there that we should be paying attention to that kill more people than Ebola has, it is the mortality rate that makes the disease scary. More than half of the people who contract Ebola die as a result of the infection. Diseases like the flu, who some say is more deadly, don’t even have a mortality rate close to that.
This is where I step on my soapbox for a moment, so get ready. . .
Last week, White House Press Secretary Josh Earnest essentially said that travel bans were off the table. He said that “the only way to eliminate risk from Ebola to the American public is to stop its outbreak at the source” meaning that the battle against Ebola needs to be fought in Africa. Mr. Earnest is partially correct. As with any outbreak like Ebola, it needs to be isolated at some level to truly be considered contained. By allowing travel into the United States from these regions with high infection numbers, we are only aiding its spread. Its source needs to be contained, and the only way to contain it at its source is to limit travel from the region that it is originating from.
Now, I say “limit” because I feel that United States citizens should be allowed to travel freely back into our country, but for the safety of the nation, right now that needs to come with some stipulations. In my opinion, the best way to limit the spread of Ebola in the United States is to quarantine anyone coming from this region for 21 days prior to releasing them into the “general public.” This goes for doctors, the military, anyone who has traveled through the region.
That is going to conclude this three part series about Ebola. I want to thank everyone who linked anything just about anywhere on Social Media (Facebook, Twitter, blogs) it all helped me gather the information that I needed to put this together.
While the hype from the mainstream media might be a bit much, I still think that there is a need to be concerned about this. Over the last seven months, the number of documented Ebola patients has increased more than five times over what was previously documented in the past forty years.
Stay vigilant, and be aware of your surroundings. The key to combating Ebola in the United States and more importantly keeping yourself safe when first contact is made with these patients is dependent on maintaining a high index of suspicion.
1. Expert: EMS’s role in the Ebola fight Author: Dr. Alex Garza October 2014
2. Case Definition for Ebola Virus Disease (EVD) Author: Center for Disease Control and Prevention September 2014
Considering we’ve had one case come over without any travel bans…I find it hard to believe a travel ban would fix anything.
Yes and no, Chris. There is talk of containment and allowing travel as freely as we do does little to assist with said containment. As I said, the most alarming thing for me is the sheer number of documented patients that have been discovered this time around… 5 times as many in this outbreak than in all of the previous outbreaks combined.
I feel like the big fear about travel bans is that we will somehow offend somebody. Well, in addition, until this is contained, instituting one would reduce the amount of fear currently being expressed state side.